Spiritual support for hospitalised COVID-19 patients during March to May 2020
by Irena Papadopoulos, Runa Lazzarino, Steve Wright, Poppy Ellis Logan, Christina Koulouglioti,
Published by the Research Centre for Transcultural Studies in Health,
Middlesex University
September 2020
Summary
This rapid exploration of available online data sought to address the following questions:
- To what extent has the provision of spiritual support for the COVID-19 hospitalised patients been covered by mass and social media and the websites of spiritual leaders/institutions and those of the NHS, in England, in the period between 20th March to 20th May?
- How has the provision of spiritual support for the COVID-19 hospitalised patients been represented within by mass and social media and the websites of spiritual leaders/institutions and those of the NHS, in England in the period between 20th March to 20th May?
- Has the COVID-19 pandemic affected how spiritual support is conceived, valued, and enacted within the NHS in England in the period between 20th March to 20th May?
- What are the lessons we can draw from the findings of this study?
Key finding, conclusions and recommendations
Towards a National Strategy for the provision of Spiritual Care and Support during Major Health Disasters.
by Irena Papadopoulos, Runa Lazzarino, Christina Koulouglioti, Sheila Ali and Steve Wright
Published by the Research Centre for Transcultural Studies in Health,
Middlesex University
September 2021
Abstract
Background
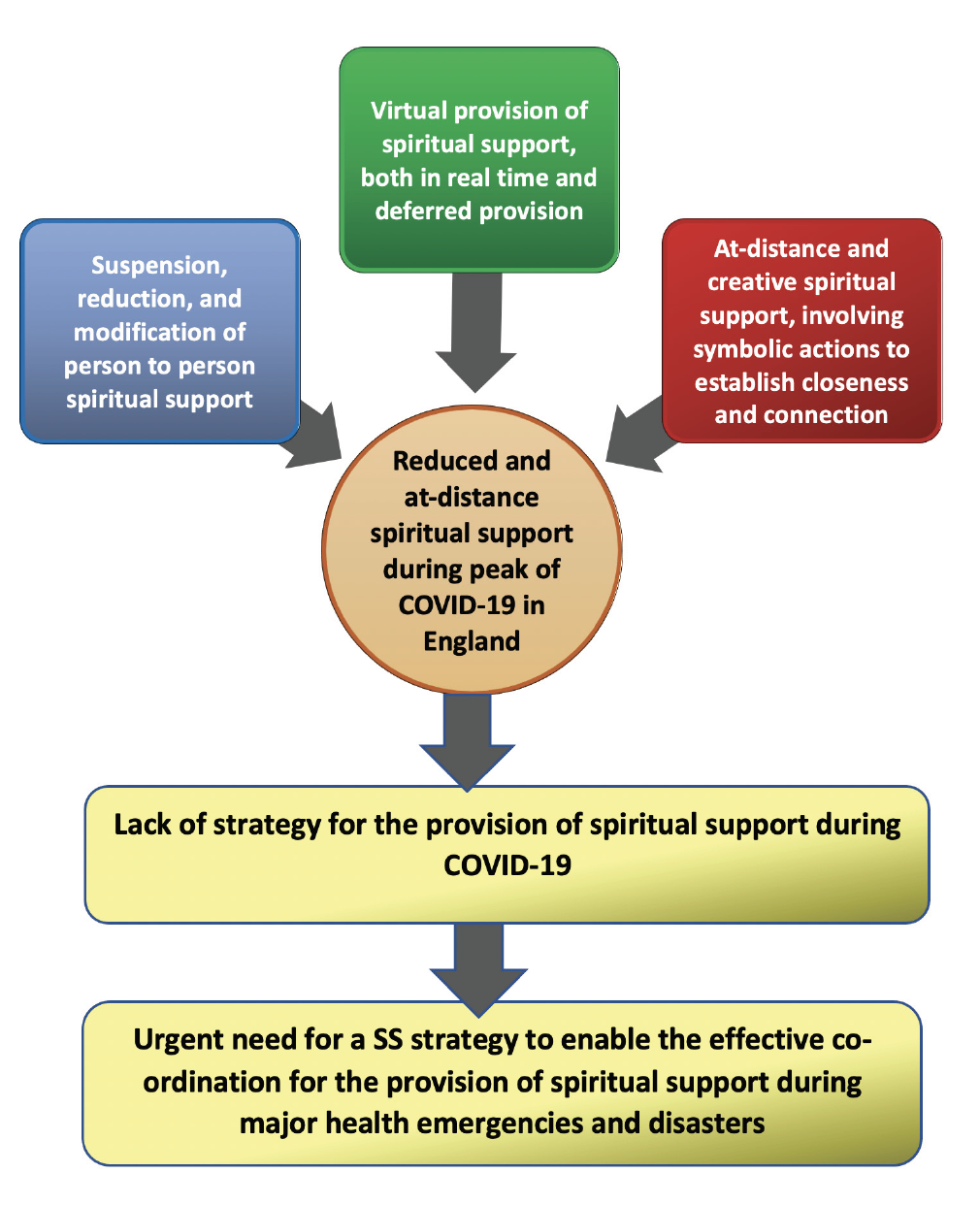
Spirituality is an integral part of being human, and should therefore be part of all fields of healthcare such as prevention, treatment, coping, recovery or death. During Major Health Disasters (MHDs), the demand for Spiritual Care and Support (SCS) grows exponentially, while the emergency burden of care and focus on preserving life often hamper its provision. The COVID-19 pandemic was an extreme global crisis, during which SCS drastically diminished, suggesting that healthcare providers and governments were unprepared in terms of a national strategy for the provision of SCS in health emergencies.
Aim
The aim of this study is to identify the components for a national strategy for the provision of SCS to patients, their families and staff during MHDs and emergencies.
Methods
A descriptive, cross-sectional, qualitative phenomenological design based on individual, semi-structured e-interviews with nursing managers and NHS/volunteer chaplains based in England was adopted. Thematic analysis of 25 e-interviews was performed based on a dialogic collaborative process. The documents shared by interviewees were analysed using a standardised form.
Results and Discussion
Results are divided into two parts. In Part I, five themes encapsulate the experiences of SCS narrated by participants, such as unpreparedness and the sense of being overwhelmed. Part II contains 11 themes which are translated into the 11 components of the proposed national strategy. The themes/components, accompanied by practical recommendations for action, are: Awareness of the past, Terminology, Community, Collaborations, Communication, Care and Spiritual Support, Training, Technology, Trust, Equality / Diversity / Inclusion, and Resources. An integrated framework approach illustrates who is responsible for: the planning and preparation of each component; the delivery and implementation of the action/resources needed; and the evaluation of the actions.
Conclusion
The need to have strategic frameworks, both national and local, that better equip a country to prevent, face, and recover from MHDs is paramount. Catering for the spiritual needs of the affected population should be a key aspect of any emergency strategy, given the centrality of SCS in healthcare, which becomes both exceptionally important and challenging in circumstances of mass fear and death.
Keywords: Spiritual care and support, major health disasters, COVID-19, England, NHS, senior nurses, chaplains, national strategy, preparedness, culturally competent and compassionate care.